
Mastitis, Plugged Ducts, and Engorgement: Understanding the Spectrum (and What to Do About It)
If you’ve ever experienced breast firmness or pain while lactating, you’ve likely heard a few different terms thrown around: engorgement, plugged ducts, and mastitis.
It can feel confusing, especially when advice ranges from “massage it out” to “you need antibiotics right away.” The truth is these aren’t separate problems, they exist on a spectrum of breast inflammation during lactation. Understanding that spectrum, how to prevent progression, and how to manage symptoms early can make all the difference in how quickly you feel better, and whether things progress to more serious mastitis.

What Is Mastitis?
Rather than thinking of plugged ducts, engorgement, and mastitis as completely different conditions, it’s more helpful to see them as progressive stages of breast inflammation:
Ductal inflammation (often called “plugged ducts”): localized swelling that narrows milk flow in one area
Engorgement: generalized fullness, swelling, and pressure in the entire breast. Think 2 rock hard shiny watermelons for breasts.
Inflammatory mastitis: worsening inflammation with systemic symptoms (flu-like feeling, along with a sore breast)
Bacterial mastitis: infection that may require antibiotics
At the root of all of these is inflammation caused by suboptimal or inconsistent milk removal.
This is a major shift from older thinking, where “plugs” were believed to be thickened milk that needed to be aggressively massaged out. We now know that deep or forceful massage can actually worsen inflammation and delay healing.

Why Do Breasts Become Full, Firm, and Painful?
When breasts feel firm like your forehead and painful, or if your breasts don’t soften after a feed/pump this is a sign that milk isn’t being removed effectively or frequently enough.
Common contributing factors include:
Shallow or ineffective latch
Poor positioning
Incorrect flange size
Inefficient pump or wearable pump
Going too long between feeds or pumping sessions
Baby sleeping longer stretches
Oral restrictions or oral anatomy differences in baby
Previous breast surgery affecting milk ducts or tissue
Rather than focusing only on the symptom alone (fullness and pain), we always want to ask: Why is milk not being removed effectively?

Common Times This Happens
When Your Milk Comes In (Days 2–5 Postpartum)
This is the most common time for engorgement.. Breasts may feel very full and tight, swollen or firm, and painful. Early support during this time can significantly impact comfort and long-term milk supply. Delayed or ineffective management can contribute to ongoing inflammation and reduced milk-making capacity.
Learning how to feed a tiny human is a HUGE learning curve. And unless you’ve done a prenatal consultation, you’re very likely asking yourself questions like how often do I need to feed my baby? How do I know if they’re getting enough to eat?
Infrequent or poor breast stimulation leading up to the onset of milk production can hit you hard as it all builds up and you wake up one morning in excruciating pain unable to get any milk out because you are so inflamed. Please I beg of you, book the prenatal consult.
When Baby Starts Sleeping Longer Stretches
As feeding patterns change, your breasts may not adjust immediately.
This can lead to:
Missed feeds or pumping sessions
Overnight fullness
Increased risk of inflammation
Anytime Milk Removal Is Disrupted
Illness, schedule changes, travel, stress, or supply fluctuations can all contribute. Even a short disruption in routine can trigger symptoms in sensitive breasts.
How Do I Treat Mastitis, Plugged Ducts, or Engorgement?
The goal is always the same: Reduce inflammation and support effective milk flow.
Modern guidance from the Academy of Breastfeeding Medicine (ABM) Mastitis Spectrum Protocol emphasizes treating mastitis as an inflammatory condition first, rather than aggressively trying to “clear a blockage.”
1. Rest
Think of this like your body recovering from a flu or sprain.
Rest helps your immune system regulate inflammation and supports healing.
Give yourself permission to slow down, reduce demands, and focus on recovery.
2. Ice (Yes—Ice!)
This often surprises parents.
Heat can be helpful when supporting letdown in a comfortable breast
But when the breast becomes firm, swollen, red, or painful, inflammation is the main issue
At this stage, cold is your friend.
Use cold compresses for 10–20 minutes after feeds or pumping sessions to reduce swelling and pain.
Think of it like a sprained ankle—you would ice it, not heat it.
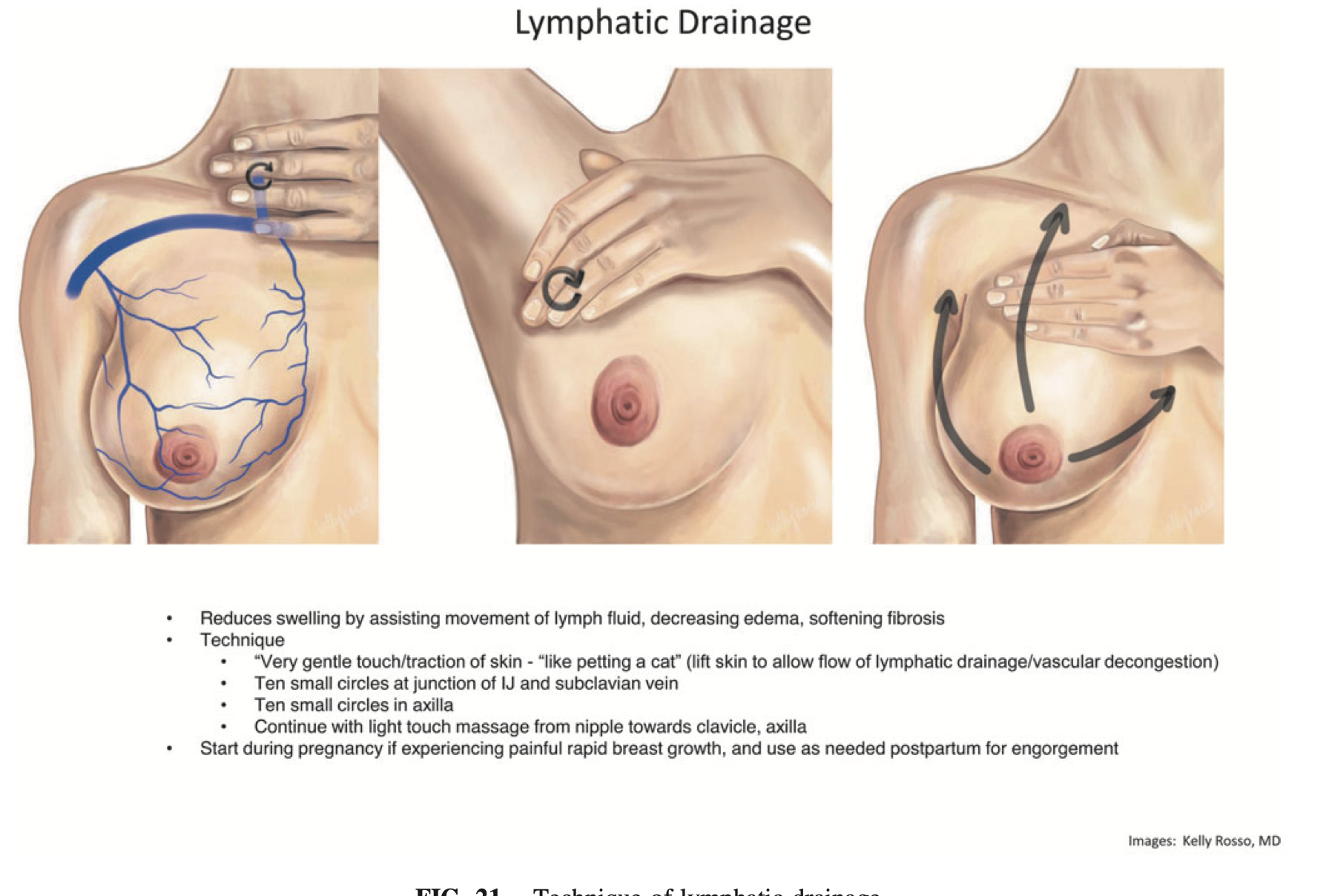
3. Lymphatic Drainage
This technique supports fluid movement and reduces swelling—similar to postpartum swelling in other parts of the body.
Key principles:
Touch should be extremely gentle (as soft as stroking a baby’s cheek)
Avoid deep tissue massage or pressure
Work in a reclined position when possible
How to do it:
Gentle circles in the armpits (10 repetitions)
Gentle circles above the collarbone (10 repetitions)
Light sweeping strokes from nipple toward the armpit and collarbone
You can also add very light tapping or “breast gymnastics” movements.
Do this for 5–10 minutes before feeding or pumping.
4. Breast Gymnastics
Originally described by IBCLC Maya Bolman, breast gymnastics involves gentle movement to support lymphatic flow and comfort.
How to do it:
Lean back
Gently move the breast side-to-side
Then up-and-down
Then in small circles (both directions)
Switch sides and repeat
This can be done before feeds or pumping sessions to encourage flow without increasing inflammation.
5. Keep Milk Moving (Without Overdoing It)
Milk removal is important, but more is not always better.
The goal is:
Effective feeds or pumping sessions
Not excessive frequency
Not “chasing empty breasts”
Over-pumping or increasing stimulation can actually increase inflammation and worsen symptoms.
When to Seek Medical Support
Contact your healthcare provider if:
Symptoms are not improving within 24 hours
Symptoms are worsening
You develop fever, chills, body aches, or flu-like symptoms along with a painful, red breast that is unbearable
This may indicate progression toward bacterial mastitis, which can require antibiotics to prevent complications such as abscess formation.
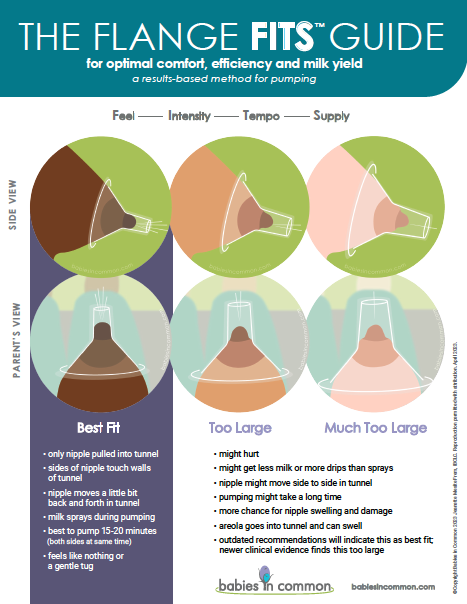
A Note on Pumping and Flange Fit
One of the most common underlying contributors I see in clinical practice is poor flange fit and use of wearable pumps.
24 mm fits NO ONE. You need to be using a flange that matches your nipple diameter and breast shape
Wearable pumps are not universally effective as primary pumps
Pumping should never be painful
You should feel breast softening after pumping
Support in Calgary
If you’re experiencing engorgement, plugged ducts, or mastitis and want hands-on support, I offer in-home lactation consultations in Calgary.
Together, we can:
Identify what’s affecting milk removal
Optimize latch or pumping
Reduce pain and inflammation quickly
Create a prevention plan tailored to your feeding journey